
In this interesting study, the authors examined the effect of geographic disparities on cataract surgery delivery to Medicare beneficiaries in the United States. Cataract extraction is the most commonly performed intraocular surgery in the United States, and Medicare beneficiaries account for approximately 80% of all cataract surgeries performed in the US. The authors analyzed Medicare claims data and US Census results to identify the number and geographic distribution of ophthalmologists delivering cataract extraction in the United States. They were able to evaluate the distance to providers for each region of the country to determine if utilization disparities exist in various regions.
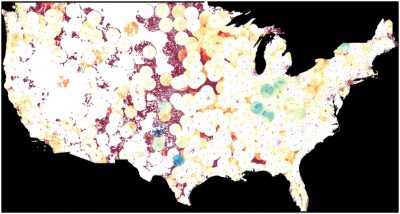
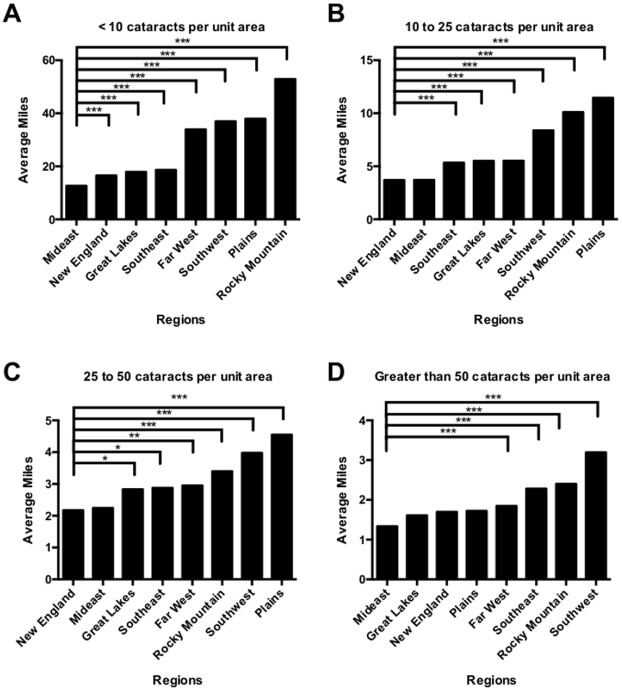
First the authors used the US census population estimates (total number and age) to project the expected number of cataract surgeries in each region. They then measured the actual number of cataract surgeries performed, and also calculated how far patients needed to travel on average by region to reach a cataract surgery provider.
Results of the analysis showed that people who live in the Plains and Rocky Mountains regions of the US must travel farther for cataract surgery compared to other regions. A significant number of expected cataract patients reside more than 100 miles from the nearest provider in Montana, South Dakota, Texas, Nevada, and Wyoming. Disparities were found between expected versus observed cataract surgery delivery across the country, but especially in the Plains and Rocky Mountains regions. Many of these utilization disparities were observed in regions with a lower density of ophthalmologists. In areas like New England and the Mideast that have a higher density of ophthalmologists, the number of expected cataract surgeries (based on age and population) closely matched the number cataract surgeries that were performed.
Travel burden is known to affect utilization in other areas of healthcare, but this study is the first to demonstrate this finding specifically for cataract care, with extensive geographic detail on distance to provider and utilization disparity across the United States. Other studies have shown that factors such as age, gender, and race can also influence the incidence of cataract and delivery of ocular care.
These findings about regional differences in access to cataract care have significant implications on future allocations of resources, especially as the population continues to age. New ideas for more efficient, cost-effective healthcare delivery throughout the United States are clearly needed.
Lee CS, Su GL, Baughman DM, Wu Y, Lee AY. Disparities in delivery of ophthalmic care; An exploration of public Medicare data. PLoS One. 2017;12(8):e0182598. doi: 10.1371/journal.pone.0182598. eCollection 2017. PubMed PMID: 28787015; PubMed Central PMCID: PMC5546578.